
Thoracic Spine Surgery
The thoracic vertebrae attach to the posterior rib cage. Commonly monitored procedures of the thoracic spine are for corrections of scoliosis and spinal deformity. These procedures involve spinal fusion, installation of steel rods and bone grafts. Other common surgery is related to trauma (compression fractures) treated with balloon kyphoplasty.
Monitoring
Typically somatosensory evoked potential (SSEP) and motor evoked potential (MEP) testing is used during scoliosis surgery. SSEPs may also prevent postoperative neuropathy or plexopathy due to patient positioning as these procedures can be quite lengthy. Injury to the thoracic spinal cord can produce abrupt bilateral or unilateral leg motor function loss as detected by MEPs and/or a decrease in lower extremity sensory functionality as detected by SSEPs. Monitoring these signals allows the surgeon to be immediately notified to prevent permanent injury. While thoracic levels are not suitable for EMG monitoring, lower thoracic and lumbar levels can utilize free running EMG testing to reduce risk to spinal nerve roots. For surgery at the level of T12-L1 the sacral nerve roots are at risk and therefore anal sphincter EMG is included in the monitoring plan.
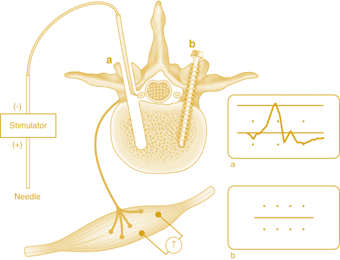
When screws are inserted into the vertebrae, triggered EMG has become a standard technique used to ensure safe placement of the screws. Triggered EMG relies on the concept that intact cortical bone should electrically insulate a properly placed screw from the adjacent nerve root. By stimulating the pedicle screw directly, a properly place screw should not elicit any muscle response below a particular threshold.